In the UKPDS, long-term benefits of early T2D control have been well described1,3,6*
Results demonstrated a Legacy Effect, in which intensive glycemic control from the time of diagnosis had a significantly greater impact on clinical outcomes than delayed control3,6
Legacy Effect of Intensive Glucose Lowering3,6

This image titled "Legacy Effect of Intensive Glucose Lowering" illustrates a study involving 3,867 adults newly diagnosed with T2D, who were randomized to receive either conventional or intensive glucose-lowering therapy. Over a 10-year period beginning in 1977, the median A1c was 7.0% in the intensive group and 7.9% in the conventional group. By 1997, although the A1c differences had diminished, the intensive group still experienced a 12% relative risk reduction (RRR) in any diabetes-related endpoint (P = 0.029). These endpoints included events such as sudden death, death from hyperglycemia or hypoglycemia, fatal or nonfatal MI, angina, heart failure, stroke, renal failure, amputation, vitreous hemorrhage, retinal photocoagulation, blindness in one eye, and/or cataract extraction.
Glycemic control defined as achieving HbA1c <7%.1
*UKPDS was designed to establish whether intensive blood glucose control reduced the risk of vascular complications. Between 1977 and 1991, 3867 eligible participants (newly diagnosed with diabetes, 25 to 65 years of age, with an FPG level >6 mmol/L on 2 mornings, 1-3 weeks apart) were randomly assigned to an intensive policy with treatment or a conventional policy with diet.3,8
†Conventional therapy defined as diet modification only. Intensive therapy defined as sulfonylurea or insulin or—in patients >120% of ideal body weight—metformin. In the intensive group, target FPG was <6 mmol/L, while in the conventional group the aim was the best achievable FPG with diet alone; drugs were added or titrated for the intensive group when above target, while rescue drugs were added to the conventional group only if there were hyperglycemic symptoms or FPG >15 mmol/L.3
Early glycemic control from the time of T2D diagnosis had a greater impact on long-term benefits3,8
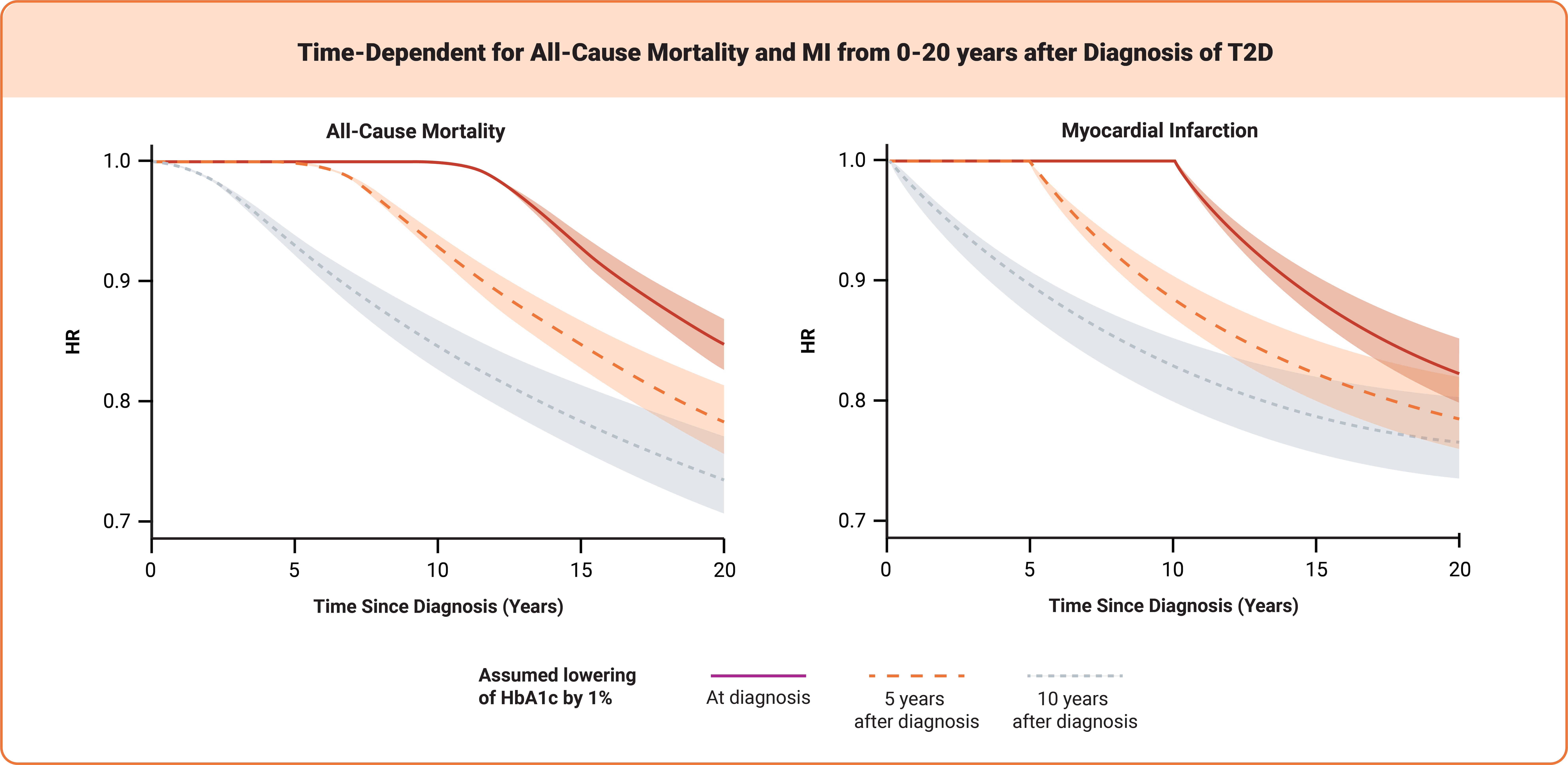
This image is titled “Time-Dependent for All-Cause Mortality and MI from 0-20 years after Diagnosis of T2D” and presents two time-dependent hazard ratio (HR) graphs illustrating the impact of a 1% reduction in A1c on all-cause mortality and myocardial infarction (MI) over a 20-year period following a diagnosis of T2D. The first graph, titled "All-Cause Mortality," plots HR on the vertical axis from 0.0 to 1.0 and Time Since Diagnosis (Years) on the horizontal axis from 0 to 20 years. The second graph, titled "Myocardial Infarction," displays HR values from 0.4 to 1.4 over the same time span. Each graph includes three curves representing the effect of A1c reduction when initiated at diagnosis, five years after diagnosis, and ten years after diagnosis.

Results demonstrated a Legacy Effect, in which lowering HbA1c by 1% soon after diagnosis had a greater impact on clinical outcomes than delayed control.8
When considering the UKPDS data, a patient like Ted who achieves early glycemic control with a proactive treatment approach is more likely to have a lower risk of T2D complications and less likely to have required escalation to insulin therapy.3,7

ADA-EASD Consensus Report:1
“Among young adults with type 2 diabetes, immediate and sustained glycemic management should be pursued, aiming for HbA1c 7% (≤53 mmol/mol) (or even lower). This presents the best opportunity to avoid complications of diabetes across the lifespan.”
What could early treatment intensification mean for Ted’s T2D management?
After early treatment intensification, Ted achieved his glycemic and weight loss goals and maintained them through his 1-year follow-up. His early success meant that he had the potential to reduce the risk of developing complications of T2D.1,2,4
Now, 10 years later, you’ve continued to treat Ted, and he has remained committed to managing his T2D.‡

10 Years Later3,6 | |
|---|---|
Ted has the potential to reduce his risk of developing microvascular complications, such as§: | Retinopathy Neuropathy Nephropathy |
He may also reduce his risk of developing macrovascular complications, such as§: | Ischemic heart disease Peripheral vascular disease Cerebrovacular disease |
10 Years Later3,6 |
|---|
Ted has the potential to reduce his risk of developing microvascular complications, such as§: Retinopathy Neuropathy Nephropathy |
He may also reduce his risk of developing macrovascular complications, such as§: Ischemic heart disease Peripheral vascular disease Cerebrovacular disease |
‡Hypothetical patient profile.
§Based on outcomes observed in UKPDS and the Diabetes and Aging study. Additional research is needed to confirm these outcomes in newer medication classes.3,7,9
Early and proactive treatment of T2D can help patients achieve their goals sooner and avoid long-term complications.1
Let's review key points for a patient like Ted from the ADA/EASD Consensus Report:
- More effective therapies with a low risk of hypoglycemia can be considered in addition to or instead of metformin from the start of T2D management1,5,6
- Weight management is an important component in T2D management, and for patients with excess weight, consider medications for glycemic control and weight management as adjuncts to lifestyle intervention1
- To avoid therapeutic inertia, reassess progress and modify treatment every 3 months if not at goal, monitoring every 6 months once goals are achieved1,5
- Achieving glycemic targets (7% or less) early after diagnosis may result in substantial and enduring reductions in the onset and progression of microvascular complications1
References
- Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753-2786. doi:10.2337/dci22-0034
- Schwartz SS, Epstein S, Corkey BE, et al. The time is right for a new classification system for diabetes: rationale and implications of the β-cell-centric classification schema. Diabetes Care. 2016;39(2):179-186. doi:10.2337/dc15-1585
- UK Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837-853. doi:10.1016/S0140-6736(98)07019-6
- DeFronzo RA. Banting Lecture. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. Diabetes. 2009;58(4):773-795. doi:10.2337/db09-9028
- Campbell IW. Need for intensive, early glycemic control in patients with type 2 diabetes. J Brit Cardiol. 2000;7:625-631.
- Holman RR, Paul SK, Bethel MA, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577-1589. doi:10.1056/NEJMoa0806470
- Matthews D, Del Prato S, Mohan V, et al. Insights from VERIFY: early combination therapy provides better glycaemic durability than a stepwise approach in newly diagnosed type 2 diabetes. Diabetes Ther. 2020;11(11):2465-2476. doi:10.1007/s13300-020-00926-7
- Lind M, Imberg H, Coleman RL, et al. Historical HbA1c values may explain the type 2 diabetes legacy effect: UKPDS 88. Diabetes Care. 2021;44(10):2231-2237. doi:10.2337/dc20-2439
- Laiteerapong N, Ham SA, Gao Y, et al. The legacy effect in type 2 diabetes: impact of early glycemic control on future complications (The Diabetes & Aging Study). Diabetes Care. 2019;42(3):416-426. doi:10.2337/dc17-1144